
What's happening to generic drug prices? - September 2018 NADAC Survey Update
It’s NADAC survey results week, which means it’s time for our second installment of “what happened to generic drug prices last month.”
As a reminder, each month retail pharmacies across the country are surveyed by Myers Stauffer (on behalf of the Centers for Medicare and Medicaid Services) on their wholesaler invoice prices. The results are then compiled and released either the third or fourth week of the following month. This week, survey results were released that reflect National Average Drug Acquisition Cost (NADAC) price changes from August. Here are our key takeaways on this week’s report:
1. Compared to the July survey, fewer generic drugs increased in price, and more generic drugs decreased in price
Figure 1 shows a histogram of price changes by percentage for the August survey results versus the July survey results. Please note that we are counting NDC Descriptions here, not NDCs. Using National Drug Code (NDC) Description normalizes for the fact that some generics have 2-3 NDCs, while others could have 20-30 NDCs. We don’t want to over-weight a drug in our analysis just because it has more NDCs.
Figure 1
Source: Data.Medicaid.gov, 46brooklyn Research
There are two key takeaways from the chart – both of which are favorable for generic deflation. First, there were 246 fewer generic drugs that experienced price increases between 0-10% in the August survey compared to the July survey. The next observation is there were 171 more generic drugs that experienced price decreases of between 10-20% in August compared to July. Fewer generics increasing, and more decreasing by double digits should be favorable for overall generic deflation.
2. August survey generic deflation was substantial using Medicaid’s Q1 2018 mix
It turns out when we apply Medicaid’s Q1 2018 prescription drug dispensing mix to the changes, the weighted August survey results were VERY favorable – we are talking nearly $220 million per year favorable! Our 46brooklyn NADAC Packed Bubble Chart can help visualize the drivers of this favorability.
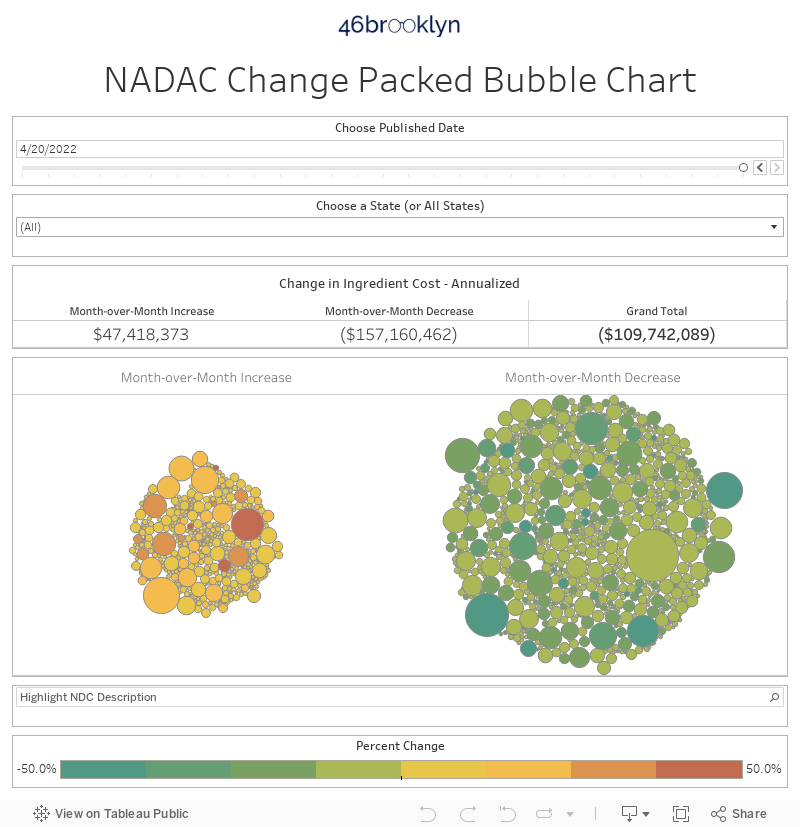
What stands out to us is not only the number of drugs that declined in price, but that there were meaningful price declines on some of the highest-spend Medicaid drugs (the large green bubbles). As shown in Figure 2 generic Tamiflu (Oseltamivir Phos 75 MG Capsule), generic Concerta (Methylphenidate ER 27, 36, 54 MG Tab), and generic Suboxone (Buprenorphine-Naloxone 8-2 MG SL) are five of the top six generic drugs that Medicaid spent money on in Q1 2018 – totalling $212 million in the quarter. These five generic drugs declined in price by an average of roughly 10% in the August survey, driving a substantial amount of actual dollar deflation on Medicaid’s drug mix.
Figure 2
Source: 46brooklyn Research
We’ll admit that using Medicaid’s Q1 2018 mix is not perfect – Tamiflu is a seasonal drug, so annualizing its deflation off of Q1 2018 volume (at the peak of flu season) is overstating the annualized impact. That said, this analysis at least gives us some comfort that the drugs that we need to get cheaper to really impact our overall spending did in fact get cheaper in August.
3. Generic Viagra (Sildenafil) got real cheap, real fast
Last month we called out generic Viagra (Sildenafil 25 MG Tablet) as one of the largest percentage decliners in the survey. This month, the 50 MG and 100 MG strengths followed suit and dropped to $0.67 per unit (97.4% decline) and $4.38 per unit (83.6% decline), respectively. Good to see the generic marketplace working so quickly!
Figure 3
Source: 46brooklyn Research
4. Generic Gleevec (Imatinib Mesylate) is down to $21 a pill
What a difference a year makes! This time last year one tablet of Imatinib Mesylate 400 MG cost your average community retail pharmacy $156. That’s now down to $21. We’re anxiously looking forward to the release of Q2 2018 Medicaid State Drug Utilization Data (expected in November, as per CMS’ FAQ - see last question) to see if states’ managed care programs are realizing these savings.
Figure 4
Source: 46brooklyn Research
5. Generic Gleevec 2.0? The price of generic Reyataz (Atazanavir Sulfate) took a nosedive in August
With more of our drug spend shifting to speciality, we feel it’s important to keep close tabs on the acquisition price of the (relatively few) specialty drugs that have gone generic. Reyataz (Atazanavir Sulfate) – a protease inhibitor indicated for use in combination with other antiretroviral agents for the treatment of HIV-1 infection - is one of these drugs, with Teva bringing the generic to market on December 27, 2017. As shown in Figure 5, the price for the generic has hovered around half the cost of the brand since its NADAC became available in early-2018. The August survey was the first nosedive the generic has experienced in price – likely due to the entrance of Aurobindo Pharma into the market – falling 43% to $13.83 per capsule.
Figure 5
Source: 46brooklyn Research
Given that Reyataz had annual sales of $402 million, this is a big deal. Our bubble chart confirms this – we show that the August change in the price of this relatively low-utilization speciality generic (only 0.0022% of overall Q1 2018 Medicaid generic units dispensed) had the fifth largest favorable impact on annualized Medicaid generic spending!

Figure 6
Source: 46brooklyn Research
It will be interesting to see what states pay for this drug within their Medicaid programs in the second half of 2018. Will this be another example of generic Gleevec, where state payments per unit become unhinged from the actual acquisition cost, or will PBMs reduce the price managed care organizations are paying for this drug generic drug in line with its NADAC? As long as payers are paying prices for generics that are linked in some way to stale Average Wholesale Prices (AWPs), we’re not betting on the latter.
What did we miss?
As always, we welcome feedback to help make our analysis more helpful for those looking to better understand the movement in drug prices. What are we missing? Please don’t hesitate to contact us to let us know.