
What’s happening to generic drug prices? March 2020 NADAC Survey Update
COVID-19 has halted a lot in the last couple weeks, but it hasn’t halted generic drug price changes. While we know your minds may be elsewhere, we believe there will be a lot to be learned about the prescription drug supply chain as the pandemic disrupts the traditional flow of medicine in the U.S. in the coming months.
CMS released its latest National Average Drug Acquisition Cost (NADAC) survey results last week. Be sure to click through our new updated visualizations (NADAC Change Packed Bubble Chart and Drug Pricing Dashboard) to see the impact of the latest changes. We have summarized the key takeaways for you in this report.
As a reminder, each month, retail community pharmacies across the country are surveyed by Myers Stauffer (on behalf of the Centers for Medicare and Medicaid Services) on their wholesaler invoice prices. The results are then compiled and released either the third or fourth week of the following month. On March 18th, survey results were released that reflect NADAC price changes from February.
Here are our top takeaways on last month’s results:
1. 30% increase in number of generics with double-digit price increases
Each month, we first look at how many generic drugs went up and down in the latest month’s survey of retail pharmacy acquisition costs, and compare that to the prior month. As shown in Figure 1, March was an interesting month. The number of generics with both single-digit increases and decreases declined – a mixed outcome. But when we look at drugs with larger, double-digit, price changes the picture looks distinctly more unsettling.
Basically, the quick way to read the chart below is to look for blue bars that are taller than orange bars to the left of the dotted line and exactly the opposite to the right of the dotted line. That would indicate a good month – more generic drugs going down in price compared to the prior month, and less drug prices going up. As shown below, the data didn’t behave that way this month.
Figure 1
Source: Data.Medicaid.gov, 46brooklyn Research
To put some numbers to this, for every generic drug that experienced a price decline in this month’s update, there were 1.19 generic drugs that experienced a price increase. That’s up from a ratio of 1.02 last month. “Up” is not good — unless you are a drug wholesaler or a generic manufacturer.
In March, there were 8% fewer generic drugs that experienced a 0-10% price decrease and 34% fewer generic drugs that experienced a price decrease of more than 10%. On the other side of the ledger, there were 7% fewer drugs that experienced a 0-10% price increase, which is good. But the most attention grabbing stat, in our view, is that there were 30% more generic drugs that experienced a price increase of more than 10%.
Note that current NADAC prices reflect surveyed pharmacy invoice costs from February. As such, they do not yet account for either real or panic-driven COVID-19 related drug shortages.
2. Weighted Medicaid generic inflation increases to $40 million
As we’ve written in prior updates, knowing the price changes alone are not enough. We need to apply utilization (drug mix) to the price changes, which is the purpose of the NADAC Change Packed Bubble Chart (embedded below). We use Medicaid’s Q4 2018 through Q3 2019 drug mix to arrive at an estimate of the total dollar impact of the latest NADAC pricing update. This helps quantify the real impact of those price changes from a payer’s perspective.
Please note that we have relaunched a cleaned up version of the NADAC Change Packed Bubble Chart this month. All of the functionality is identical to the original version, it should just be a bit more intuitive to use, and display a bit better on most screens. If you are accessing using your phone, please flip it sideways to view in landscape.
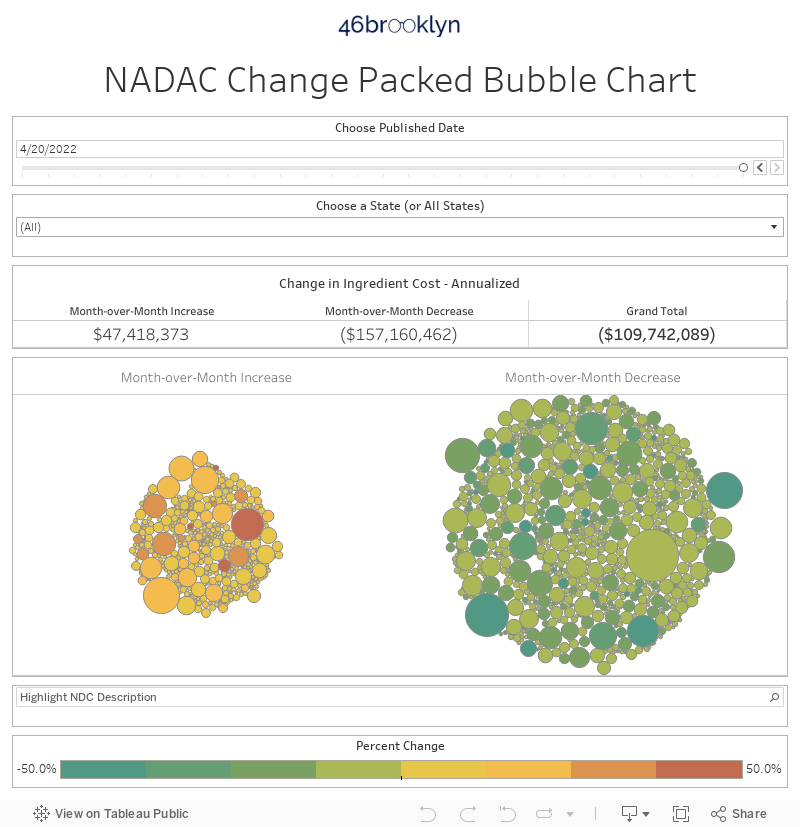
The green bubbles on the right of the above viz are the generic drugs that experienced a price decline in the latest survey, while the yellow/orange/red bubbles on the left are those drugs that experienced a price increase. The size of each bubble represents the dollar impact of the drug on Medicaid, based on utilization of the drug in the most recent trailing 12-month period. Stated differently, we simply multiply the latest survey price change by aggregate drug utilization in Medicaid over the past year, add up all the bubbles, and we get the total inflation/deflation impact of the survey changes.
Put it all together, and the weighted impact to Medicaid of the latest monthly survey was $40 million of generic inflation (the second consecutive month of generic drug inflation).
3. Year-over-year generic oral solid deflation drops under 7%
As shown in Figure 2, year-over-year deflation on generic oral solids (orange line) hit a two-year low this month, registering 6.8%. We’ve added a new line to the chart, showing the YoY deflation on ALL generic drugs. Deflation on this broader population of drugs is also at a two-year low, down to only 4.8%. Please note that the trailing 24-month Average and +/1 standard deviation lines are still based on the “oral solid” data series in the below chart.
Figure 2
Source: Data.Medicaid.gov, 46brooklyn Research
Keep in mind, that back in mid-2019, alarm bells went off that the generic drug marketplace was underperforming at its worst levels in two years. Fast-forward to today, and it appears that it was just the beginning of an overall neutering of generic drug deflation. Effectively, over the last few months, the mechanisms that traditionally work to drive generic drug prices down have been sheltered in place.
4. Naproxen (delayed release) shoots up 803%
Within the NADAC Change Packed Bubble Chart, the darkest red bubbles represent the drugs that experienced the largest month-over-month price increase, while the largest bubbles represent the drugs that had the greatest ingredient cost impact to Medicaid. It’s not often that one of the largest bubbles is also the darkest red bubble.
This happened this month, as naproxen DR 500 mg tablets (i.e. generic Naprosyn) rocketed up from $0.23 per pill to $2.07 per pill. Figure 3 (below) shows this month’s spike, compared to the price of the older intermediate release version of naproxen 500 mg tablets. This pricing spike translates to $6.5 million in higher annual ingredient costs across Medicaid programs.
Figure 3
Source: Data.Medicaid.gov, Elsevier Gold Standard Drug Database (GSDD), 46brooklyn Research
As a quick aside, for those of you that have used our NADAC Drug Pricing Dashboard in the past, you may notice that Figure 3 looks a bit different than it used to. We recently republished this seminal 46brooklyn dashboard, complete with a new clinical drug information backbone using Elsevier’s Gold Standard Drug Database (GSDD). GSDD fixes the #1 problem we had with the FDA’s data – namely that generic names are oftentimes duplicated and littered with misspellings. Because of this, we had to allow you to select multiple generic drug names at a time – not ideal from a usability standpoint. Through leveraging GSDD, we have eliminated this problem, making it considerably easier to find the drug for which you are looking. If you have a moment, take a look at the updated dashboard and let us know what you think.
Also, late last week, at the same time everyone was rushing to 46brooklyn to read our 2018 hydroxychloroquine report, we published another dashboard called the Abnormal Drug Price Increase Tracker (ADPIT). ADPIT is designed to immediately identify price movements like this one on naproxen, flagging them for the drug pricing and shortage research communities to investigate further. Navigate over to our ADPIT tool and sort the table by “Relative Impact Ratio” (which is the current price divided by the 90th percentile price over the past 52 weeks – see our full report covering both this new tool and our Medicaid Drug Market Share Dashboard relaunch for more details), and you’ll see all of the naproxen DR strengths at the top of the list (Figure 4):
Figure 4
Source: Data.Medicaid.gov, 46brooklyn Research
5. Gleeve-zy come, Gleeve-zy go
Last month, we wrote about generic Gleevec’s big drop to $5.81 per pill, bringing the annual ingredient cost for a course of treatment down to roughly $2,100 per year. Well, as shown in Figure 5, this month generic Gleevec (imatinib mesylate) nearly doubled to $11.67 per pill.

Figure 5
Source: Data.Medicaid.gov, Elsevier Gold Standard Drug Database (GSDD), 46brooklyn Research
However, what’s interesting about this drug is that it doesn’t show up in our ADPIT tool this week. This means that a doubling in the price of imatinib was not technically abnormal, at least relative to this drug’s extreme historical volatility. This conceptually makes sense when we look at the above chart. On inspection of the chart, it very much “feels” that this latest pricing move was well within the drug’s normal volatility range. ADPIT allows us to transition from relying on feel to relying on math. It tells us that yes, this latest pricing move, despite the unexpected sticker shock we may get, should not have been totally unexpected. It tells us that we perhaps overreacted to last month’s drop in price, and warns us not to do the same this month.
Herein lies the power of this new tool. It protects us from our very limited human brains, which want to see trends everywhere (when many times they aren’t really there) and overstate the importance of latest “hot” information (a.k.a. “recency bias”). In short, tools like ADPIT inject a healthy dose of fact and math at a time when we are in desperate need of both.
A call for help
Now more than ever, we need to hear from you. Knock-on effects from COVID-19 are creating the following problems:
The push for more 90-day fills, putting pressure on supply chain inventories;
Prescribers playing Hungry Hungry Hippos with vital drug supply;
The likelihood of supply chain disruptions leading to more shortages;
Rampant twitter-speculation on COVID-19 treatment drugs, sparking runs on several common generic medications in use globally for other indications
Our role is to follow the data, but public data is not keeping up with the pace at which the drug inventories in this country are fluctuating. As such, much of our time is now devoted to putting our ear to the ground to gain a better understanding of how our drug supply chain is coping with the unprecedented stress it is facing. So pharmacists, please let us know what you are seeing. We are working to responsibly provide this information to the public so that patients, journalists, policymakers, and researchers can be better equipped to meet this new challenge.
To all the policymakers, journalists, and thought-leaders out there, if we have learned anything over the past two weeks, it’s that words have a heightened power amidst this crisis. A citizenry desperate for answers and hope is ready to cling to whatever they can get their hands on. From cleaning supplies to immunosuppressive drugs, fear and hope can empty shelves in stores and behind the pharmacy counter. And while there are interesting methods of adapting to things like toilet paper shortages, unfortunately when it comes to medicine, patients with life-threatening diseases often can’t improvise.
We implore those with sizable followings to take extra care with information when sharing with those who are anxious to overdose on it. Tempering leading messages, being cognizant of how messages might be digested, and being thorough with message context are essential ways to ensure that information-sharing won’t do more harm than good.
The team at 46brooklyn would like to extend our thanks to everyone who is working to find solutions and treatments for the pandemic we’re faced with. We have faith in the combination of the drug industry, our nation’s army of medical experts, and government officials that we will have a solution before long. But it is imperative that we make the road as smooth as possible – which isn’t done with false hope, incorrect information, and misleading guidance. There are enough lives on the line with the pandemic alone. It’s incumbent on all of us to make sure we’re not adding to the problem, but working to mitigate it.
Big shout-out to Sara Talpos at Undark for her excellent deep-dive on the explosion of interest in hydroxychloroquine as a possible treatment for COVID-19 despite its unproven efficacy, and how the overhype is leading to overprescribing, hoarding, and shortages that threaten to harm those who regularly rely on the treatment.