
What’s happening to generic drug prices? September 2019 NADAC Survey Update
Hi there again, drug pricing aficionados. Good news. CMS recently released their latest NADAC survey results, which means it’s time to check in on the September generic drug price changes.
There was a lot of movement on drug prices last month, so be sure to click through our new updated visualizations (NADAC Change Packed Bubble Chart and Drug Pricing Dashboard) to see the impact.
As a reminder, each month, retail community pharmacies across the country are surveyed by Myers Stauffer (on behalf of the Centers for Medicare and Medicaid Services) on their wholesaler invoice prices. The results are then compiled and released either the third or fourth week of the following month. On September 18th, survey results were released that reflect National Average Drug Acquisition Cost (NADAC) price changes from August. Here are our top takeaways on the results:
1. September unweighted price change histogram slightly worse than August
Each month, we first look at how many generic drugs went up and down in the latest month’s survey of retail pharmacy acquisition costs, and compare that to the prior month. As shown in Figure 1, September looked a whole lot like August – more drugs decreased in price than increased in price.
Figure 1
Source: Data.Medicaid.gov, 46brooklyn Research
To put some numbers to this, for every generic drug that experienced a price decline this month, there were only 0.83 generic drugs that experienced a price increase. That’s slightly up from a ratio of 0.79 last month.
In September, there were 3% more generic drugs that experienced a 0-10% price decrease, but 5% fewer generic drugs that experienced a price decrease of more than 10%. Also, there were 8% more drugs that experienced a 0-10% price increase, and 2% more drugs that experienced a price increase of more than 10%.
2. This month brought $41 million of annualized deflation using Medicaid’s drug mix
As we’ve written in prior updates, knowing the price change alone is not enough. We need to apply utilization (drug mix) to the price changes, which is the purpose of the NADAC Change Packed Bubble Chart (embedded below). We use Medicaid’s 2018 drug mix to arrive at an estimate of the total dollar impact of the latest NADAC pricing update. This helps quantify the real impact of those price changes from a payer’s perspective.
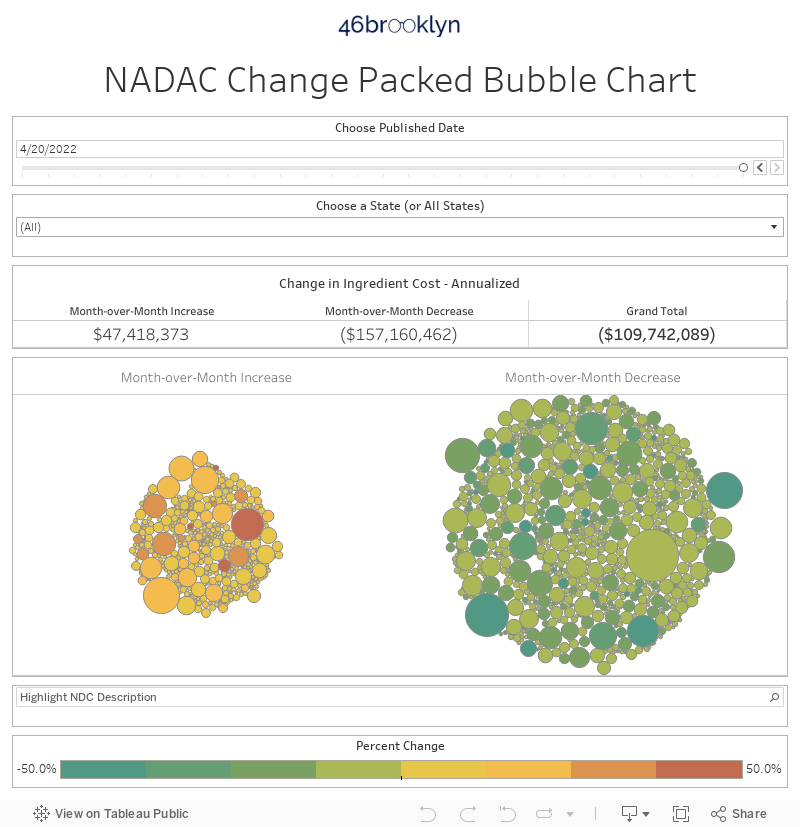
The green bubbles on the right are the generic drugs that experienced a price decline in the latest survey, while the yellow/orange/red bubbles on the left are those drugs that experienced a price increase. The size of each bubble represents the annualized weighted impact of the drug on Medicaid – i.e. we multiply the survey price change by aggregate drug utilization in Medicaid. Add up all the bubbles and we get the total annualized inflation/deflation. This month, it was a more modest but still meaningful $41 million in annualized deflation.
3. Year-over-year deflation bounces back down to 11.8%
Trailing-twelve-month generic deflation was 11.8% this month, about 3% worse than the deflation over the past 24-months. It seems that the June Gloom has returned as the back-to-school blues.
Based on Figure 2, it’s sure starting to look like generic deflation is resetting in a new, lower range. But it’s still much too early to make that call. We’ll keep updating this each month and see where it goes!
If you’re curious about how we created this chart, take a look at our June 2019 NADAC survey report for more detail on our methodology.

Figure 2
Source: Data.Medicaid.gov, 46brooklyn Research
4. Well, well, well … generic Wellbutrin XL prices fall by more than 20%
Prices for generic Wellbutrin XL (buproprion XL tablet), a medication indicated for major depressive disorder and seasonal affective disorder, had been climbing for much of 2019. But this past month saw a strong 34% decline for buproprion XL 300 mg, moving from $0.47 per tablet to $0.31 per tablet (Figure 3).
Figure 3
Source: Data.Medicaid.gov, 46brooklyn Research
This translates into approximately $5 less per prescription per month based upon typical dosing or $6,000 in annualized savings for every 100 patients taking this medication chronically over a year.
5. Prices spike on generic Pyridium by more than 50%
This past month saw some large sudden price spikes on both strengths of generic Pyridium (phenazopyridine tablet), a pain reliever typically used for urinary tract infection.
The 100 mg version of phenazopyridine shot up 60%, which amounted to 25 cents per tablet, and the 200 mg version of phenazopyridine spiked 56.9%, which amounted to 41 cents per tablet (Figure 4).
Figure 4
Source: Data.Medicaid.gov, 46brooklyn Research
These price increases amount to a whopping $1.8 million in annualized spending increases for state Medicaid programs.
6. Generic Concerta jumps again … and leads to the development of a new volatility measure for generic drugs!
As we’ve talked about here and here and here, generic Concerta (methylphenidate ER) prices continue to be a roller coaster ride in the generic drug market. This month, the most commonly dispensed strength of methlyphenidate ER (36 mg) shot up 21%, forming the tumor that you probably noticed disgracefully hanging off of the side of the latest month’s bubble chart (scroll up to section 2 if you missed it!).
Let’s be honest, it’s probably getting old reading about this drug bouncing up and down with little insight from us on why. It’s sure getting old writing about it without adding any value.
So this month, we decided to look at this generic drug through a new angle – its pricing volatility. For those of you in the financial markets, this will be a very familiar concept. A financial security’s price is usually what gets all the attention, but just as critical when evaluating a security is its volatility (for options … delta, gamma, theta - a.k.a. “the greeks”). Price measures the “reward” while volatility measures the “risk.” They are like the yin and yang of financial management.
So it’s about time we introduced this concept to drug pricing analysis. It’s actually quite appropriate given how many parallels there are between how the members of the drug supply chain and Wall Street traders operate. Both make money by finding (or creating) opaque markets with massive information asymmetry (where they know more than their trading partners) and then buying low and selling high over and over again. In such scenarios, the more volatility there is in a security (or a drug), the more opportunities there are to make money. As such, we better start understanding drug price volatility.
To measure generic drug price volatility, we borrowed a statistical technique called “coefficient of variation (CV),” or “relative standard deviation (RSD).” From here on out, we’ll shamelessly re-brand CV/RSD within our research as Generic Price Volatility (GPV).
To come up with GPV, we calculated the standard deviation of the most recent 12-months of prices for every distinct generic drug that had at least 12-months of NADAC price history (a total of 3,243 generic drugs). We then divided this standard deviation by the mean NADAC price of each drug over the same 12-month period. We then collected all drugs and threw them into a histogram (Figure 5).
Figure 5
Source: Data.Medicaid.gov, 46brooklyn Research
Figure 5 displays the number of generic drugs that fall into each GPV “bucket.” For example, the bar all the way to the left tells us that there are 187 drugs that – based on their last 12 months of NADAC prices – have a GPV between 0% and 2%. Overall, the median GPV of the three-thousand-plus generic drugs in the population is 6.2%.
If you were wondering what a GPV of less than 2% looks like, look no further than the old reliable drug you take for your run-of-the-mill infections – amoxicillin 500 mg capsule. As shown in Figure 6, this generic “patient” has flat-lined.
Figure 6
Source: Data.Medicaid.gov, FDA.gov, 46brooklyn Research
You may also be wondering what a high GPV drug looks like. Figure 7 shows tetracycline 250 mg capsule, a drug we have written about in the past, which we now know sports a healthy 26.5% GPV owing to its predisposition to wander aimlessly between ~$1.75 and ~$3.50 per capsule over the past year.
Figure 7
Source: Data.Medicaid.gov, FDA.gov, 46brooklyn Research
But the reason we did this in the first place was to understand if methylphenidate ER 36’s volatility is completely out of line with the rest of generic drugs. It turns out the answer is yes, but not as much as we suspected. Methylphenidate ER 36 mg tablets have a GPV of 12.9%, which puts it in the 84th percentile among all generic drugs. To be fair, that’s pretty high relative volatility … but its not as bad as we suspected. With the giant methylphenidate circles commonly showing up on either side of our bubble chart viz ledger each month, we were bracing ourselves for much worse.
Note: This is not the last time we will discuss volatility and our newly coined “GPV” concept. A visualization is in the works … stay tuned!
7. A whole lot of generic Concerta!
It turns out that the problem with this drug is not just its volatility – the problem is its volatility plus its high price plus its enormous Medicaid utilization. To illustrate this, we’ve isolated all of the generic drugs with a GPV similar to methylphenidate ER 36mg tablet (in the 80th to 90th percentile). Figure 8 shows the Total Amount Reimbursed by all payers in Medicaid on each of the top 10 drugs in this group. It spent almost as much on methylphenidate ER 36 mg as it did on the next nine generic drugs COMBINED.
Figure 8
Source: Data.Medicaid.gov, 46brooklyn Research
So this leads to the natural question of why is Medicaid covering so much of this high-cost, high-volatility drug? As we have written in the past, this is the most common generic drug/strength used to treat ADHD. Knowing that, the deeper question is whether we are over-dispensing all ADHD medications?
We set out to explore this question, but unfortunately were not able to come up with a definitive answer. But the work we did may still be useful to those of you out there that are able to devote more time and expertise than we can to ADHD drug utilization research, so we’ll go ahead and share what we found anyway.
7. Burrowing deeper into the ADHD drug rabbit hole…
According to Medicaid.gov, between 2014 and 2018 there was an average of about 72.1 million folks eligible for Medicaid and CHIP each month. Over the same period, there were 3.5 billion units of all DEA Schedule II ADHD treatment drugs dispensed in Medicaid. This translates to an average of 10 pills (or possibly, patches) per person per year. When looking at the dollars, Medicaid spent just over $14.5 billion on ADHD treatment drugs over this period (pre-rebate). That translates to an average of $40.23 per person per year. As shown in Figure 9, both the dollars and volume per Medicaid eligible increased through 2017 and then stepped down in 2018.

Figure 9
Source: Data.Medicaid.gov, 46brooklyn Research
Without any further context, it’s hard to determine if this is good or bad. It’s more just food for thought. For those with even hungrier brains, some additional food for thought is that both Concerta and Oxycontin are Schedule II narcotics, According to the DEA, “Substances in this schedule have a high potential for abuse which may lead to severe psychological or physical dependence.” So essentially, on average, we’re setting aside $40 per year for every single eligible Medicaid member to treat ADHD with drugs that the DEA classifies as just as addictive as high-powered opioids.
To provide some context, we replicated the above chart for Schedule II opioids. As shown in Figure 10, both the units dispensed and dollars spent have been in free fall – dropping 37% and 54%, respectively, between 2015 and 2018. In 2018, there were still more Schedule II opioid units dispensed per member (15.7) than Schedule II ADHD treatment drugs (9.7), but the gap is rapidly closing. In 2018, Medicaid spent just $7.85 per member on Schedule II opioids, compared to $40.48 per member on Schedule II ADHD treatment drugs (pre-rebate).
Figure 10
Source: Data.Medicaid.gov, 46brooklyn Research
Please don’t hesitate to reach out to us if you have any ideas on additional analysis we can do on ADHD treatment drug utilization. We are clearly intrigued by this topic and could use any help we can get in advancing our analysis on it.
What are you seeing?
While we spend more time than we’d like to admit studying the pricing changes during each NADAC Survey Results Week, we don’t always catch every story worth noting. Be sure to take a gander at all of our updated Visualizations that rely on NADAC prices. If you’re seeing any interesting movement on drugs in the dataset, let us know.
We’d like to give a special shout-out to the Side Effects team over at the Columbus Dispatch, who are peeling the latest layer in the drug supply chain. In September, they utilized 46brooklyn dashboards to examine what happened to specialty drug prices in Ohio after the state banned spread pricing in the Medicaid program. Unsurprisingly, after spread disappeared, pharmacy margins jumped on many generic specialty medications. As a follow-up editorial correctly opined, “Fixing one problem doesn’t mean true reform.” The Dispatch continues to lead the nation in exposing the dark corners of the broken drug pricing system.
46brooklyn live and in the flesh!
On October 7, 46brooklyn’s Antonio Ciaccia will be discussing our work on Medicaid pharmacy data at the Western Medicaid Pharmacy Administrators Association Conference in Idaho.
On October 23, 46brooklyn’s Eric Pachman will be speaking on a population health panel at the JAX Healthcare Forum in Farmington, Connecticut.
On October 28, Pachman will also be speaking about drug pricing reform at the National Community Pharmacists Association Annual Convention in San Diego.